


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of action: Ultibro Breezhaler: When indacaterol and glycopyrronium are administered together in Ultibro Breezhaler, they provide additive efficacy due to their different mode of action targeting different receptors and pathways to achieve smooth muscle relaxation. Due to the differential density of beta2-adrenoceptors and M3-receptors in central versus peripheral airways, beta2-agonists should be more effective in relaxing peripheral airways, whilst an anticholinergic compound may be more effective in central airways.
Thus, for bronchodilation in both peripheral and central airways of the human lung a combination of a beta2-adrenergic agonist and a muscarinic antagonist may be beneficial.
Indacaterol: Indacaterol is a long-acting beta2-adrenergic agonist for once-daily administration. The pharmacological effects of beta2-adrenoceptor agonists, including indacaterol, are at least in part attributable to stimulation of intracellular adenyl cyclase, the enzyme that catalyses the conversion of adenosine triphosphate (ATP) to cyclic-3', 5'-adenosine monophosphate (cyclic AMP). Increased cyclic AMP levels cause relaxation of bronchial smooth muscle. In vitro studies have shown that indacaterol has multi-fold greater agonist activity at beta2-receptors compared to beta1 and beta3-receptors.
When inhaled, indacaterol acts locally in the lung as a bronchodilator. Indacaterol is a partial agonist at the human beta2-adrenergic receptor with nanomolar potency.
Although beta2-adrenergic receptors are the predominant adrenergic receptors in bronchial smooth muscle and beta1-adrenergic receptors are the predominant receptors in the human heart, there are also beta2-adrenergic receptors in the human heart comprising 10% to 50% of the total adrenergic receptors. Their presence in the heart raises the possibility that even highly selective beta2-adrenergic agonists may have cardiac effects.
Glycopyrronium: Glycopyrronium is an inhaled long-acting muscarinic receptor antagonist (anticholinergic) for once-daily maintenance bronchodilator treatment of COPD. Parasympathetic nerves are the major bronchoconstrictive neural pathway in airways, and cholinergic tone is the key reversible component of airflow obstruction in COPD. Glycopyrronium works by blocking the bronchoconstrictor action of acetylcholine on airway smooth muscle cells, thereby dilating the airways.
Glycopyrronium bromide is a high affinity muscarinic receptor antagonist. A greater than 4-fold selectivity for the human M3 receptors over the human M2 receptor has been demonstrated using radioligand binding studies.
Pharmacodynamic effects: The combination of indacaterol and glycopyrronium in Ultibro Breezhaler showed a rapid onset of action within 5 minutes after dosing. The effect remains constant over the whole 24-h dosing interval.
The mean bronchodilator effect derived from serial FEV1 measurements over 24 h was 320 ml after 26 weeks of treatment. The effect was significantly greater for Ultibro Breezhaler, when compared to indacaterol, glycopyrronium or tiotropium alone (difference 110 ml, for each comparison).
There was no evidence for tachyphylaxis to the effect of Ultibro Breezhaler over time when compared to placebo or its monotherapy components.
Effects on heart rate: Heart rate effects in healthy volunteers were investigated after a single dose of 4 times the recommended therapeutic dose of Ultibro Breezhaler administered in four dose steps each separated by one hour and compared to the effects of placebo, indacaterol, glycopyrronium and salmeterol.
The largest time-matched heart rate increase compared to placebo was +5.69 bpm (90% CI [2.71, 8.66]), the largest decrease was -2.51 bpm (90% CI [-5.48, 0.47]). Overall, the effect on heart rate over time did not show a consistent pharmacodynamic effect of Ultibro Breezhaler.
Heart rate in COPD patients at supratherapeutic dose levels was investigated. There were no relevant effects of Ultibro Breezhaler on mean heart rate over 24 h and heart rate assessed after 30 minutes, 4 h and 24 h.
QT interval: A thorough QT (TQT) study in healthy volunteers with high doses of inhaled indacaterol (up to twice the maximum recommended therapeutic dose) did not demonstrate a clinically relevant effect on the QT interval. Similarly, for glycopyrronium no QT prolongation was observed in a TQT study after an inhaled dose of 8 times the recommended therapeutic dose.
The effects of Ultibro Breezhaler on QTc interval were investigated in healthy volunteers after inhalation of Ultibro Breezhaler up to 4 times the recommended therapeutic dose in four dose steps each separated by one hour. The largest time-matched difference versus placebo was 4.62 ms (90% CI 0.40, 8.85 ms), the largest time-matched decrease was -2.71 ms (90% CI -6.97, 1.54 ms), indicating that Ultibro Breezhaler had no relevant impact on the QT interval, as was expected by the properties of its components.
In COPD patients, supratherapeutic doses between 116 micrograms/86 micrograms and 464 micrograms/86 micrograms of Ultibro Breezhaler showed a higher proportion of patients with QTcF increases vs. baseline between 30 ms and 60 ms (ranging from 16.0% to 21.6% vs. 1.9% for placebo), but there were no QTcF increases >60 ms from baseline. The highest dose level of 464 micrograms/86 micrograms Ultibro Breezhaler also showed a higher proportion of absolute QTcF values >450 ms (12.2% vs. 5.7% for placebo).
Serum potassium and blood glucose: In healthy volunteers, after the administration of 4 times the recommended therapeutic dose of Ultibro Breezhaler, the effect on serum potassium was very small (maximal difference -0.14 mmol/l when compared to placebo). The maximal effect on blood glucose was 0.67 mmol/l.
Clinical efficacy and safety: The Ultibro Breezhaler clinical Phase III development programme included six studies in which over 8,000 patients were enrolled: 1) a 26-week placebo- and active-controlled (indacaterol once daily, glycopyrronium once daily, open-label tiotropium once daily) study; 2) a 26-week active-controlled (fluticasone/salmeterol twice daily) study; 3) a 64-week active-controlled (glycopyrronium once daily, open-label tiotropium once daily) study; 4) a 52-week placebo-controlled study; 5) a 3-week placebo- and active-controlled (tiotropium once daily) exercise tolerance study; and 6) a 52-week active-controlled (fluticasone/salmeterol twice daily) study.
In four of these studies, patients were enrolled who had a clinical diagnosis of moderate to severe COPD. In the 64-week study patients were enrolled who had severe to very severe COPD with a history of ≥1 moderate or severe COPD exacerbation in the previous year. In the 52-week active-controlled study, patients were enrolled who had moderate to very severe COPD with a history of ≥1 moderate or severe COPD exacerbation in the previous year.
Effects on lung function: Ultibro Breezhaler showed clinically meaningful improvements in lung function (as measured by the forced expiratory volume in one second, FEV1) in a number of clinical studies. In Phase III studies, bronchodilator effects were seen within 5 minutes after the first dose and were maintained over the 24-hour dosing interval from the first dose. There was no attenuation of the bronchodilator effect over time.
The magnitude of the effect was dependent on the degree of reversibility of airflow limitation at baseline (tested by administration of a short-acting muscarinic antagonist bronchodilator and a short-acting beta2-agonist bronchodilator): Patients with the lowest degree of reversibility at baseline (<5%) generally exhibited a lower bronchodilator response than patients with a higher degree of reversibility at baseline (≥5%). At 26 weeks (primary endpoint), Ultibro Breezhaler increased trough FEV1 by 80 ml in patients (Ultibro Breezhaler n=82; placebo n=42) with the lowest degree of reversibility (<5%) (p=0.053) and by 220 ml in those patients (Ultibro Breezhaler n=392, placebo n=190) with a higher degree of reversibility at baseline (≥5%) compared to placebo (p<0.001).
Trough and peak FEV1: Ultibro Breezhaler increased post-dose trough FEV1 by 200 ml compared to placebo at the 26-week primary endpoint (p<0.001) and showed statistically significant increases compared to each monotherapy component treatment arm (indacaterol and glycopyrronium) as well as the tiotropium treatment arm, as shown in the Table 1 as follows.
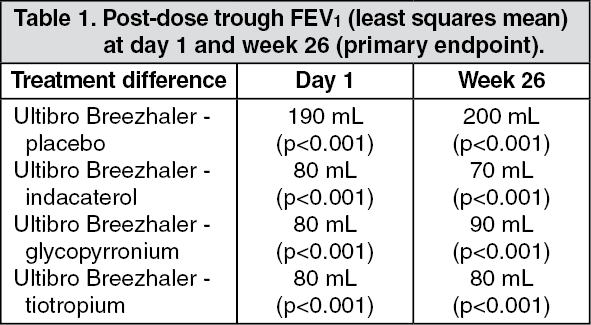 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe mean pre-dose FEV1 (average of the values taken at -45 and -15 minutes prior to the morning dose of study medication) was statistically significant in favour of Ultibro Breezhaler at week 26 compared to fluticasone/salmeterol (least squares [LS] mean treatment difference 100 ml, p<0.001), at week 52 compared to placebo (LS mean treatment difference 189 ml, p<0.001) and at all visits up to week 64 compared to glycopyrronium (LS mean treatment difference 70-80 ml, p<0.001) and tiotropium (LS mean treatment difference 60-80 ml, p<0.001). In the 52-week active-controlled study, the mean pre-dose FEV1 was statistically significant in favour of Ultibro Breezhaler at all visits up to week 52 compared to fluticasone/salmeterol (LS mean treatment difference 62-86 ml, p<0.001). At week 26, Ultibro Breezhaler produced statistically significant improvement in peak FEV1 compared to placebo in the first 4 hours post-dose (LS mean treatment difference 330 ml) (p<0.001).
FEV1 AUC: Ultibro Breezhaler increased post-dose FEV1 AUC0-12 (primary endpoint) by 140 ml at 26 weeks (p<0.001) compared to fluticasone/salmeterol.
Symptomatic outcomes: Breathlessness: Ultibro Breezhaler statistically significantly reduced breathlessness as evaluated by the Transitional Dyspnoea Index (TDI); it demonstrated a statistically significant improvement in the TDI focal score at week 26 compared to placebo (LS mean treatment difference 1.09, p<0.001), tiotropium (LS mean treatment difference 0.51, p=0.007) and fluticasone/salmeterol (LS mean treatment difference 0.76, p=0.003). Improvements versus indacaterol and glycopyrronium were 0.26 and 0.21, respectively.
A statistically significantly higher percentage of patients receiving Ultibro Breezhaler responded with a 1 point or greater improvement in the TDI focal score at week 26 compared to placebo (68.1% and 57.5% respectively, p=0.004). A higher proportion of patients demonstrated clinically meaningful response at week 26 on Ultibro Breezhaler as compared to tiotropium (68.1% Ultibro Breezhaler versus 59.2% tiotropium, p=0.016) and fluticasone/salmeterol (65.1% Ultibro Breezhaler versus 55.5% fluticasone/salmeterol, p=0.088).
Health-related quality of life: Ultibro Breezhaler has also shown a statistically significant effect on health-related quality of life measured using the St. George's Respiratory Questionnaire (SGRQ) as indicated by a reduction in SGRQ total score at 26 weeks compared to placebo (LS mean treatment difference -3.01, p=0.002) and tiotropium (LS mean treatment difference -2.13, p=0.009) and reductions versus indacaterol and glycopyrronium were -1.09 and -1.18, respectively. At 64 weeks, the reduction compared to tiotropium was statistically significant (LS mean treatment difference -2.69, p<0.001). At 52 weeks, the reduction compared to fluticasone/salmeterol was statistically significant (LS mean treatment difference -1.3, p=0.003).
A higher percentage of patients receiving Ultibro Breezhaler responded with a clinically meaningful improvement in SGRQ score (defined as a decrease of at least 4 units from baseline) at week 26 compared to placebo (63.7% and 56.6% respectively, p=0.088) and tiotropium (63.7% Ultibro Breezhaler vs. 56.4% tiotropium, p=0.047), at week 64 compared to glycopyrronium and tiotropium (57.3% Ultibro Breezhaler versus 51.8% glycopyrronium, p=0.055; versus 50.8% tiotropium, p=0.051, respectively), and at week 52 compared to fluticasone/salmeterol (49.2% Ultibro Breezhaler vs. 43.7% fluticasone/salmeterol, odds ratio: 1.30, p<0.001).
Daily activities: Ultibro Breezhaler demonstrated a statistically superior improvement versus tiotropium in the percentage of "days able to perform usual daily activities" over 26 weeks (LS mean treatment difference 8.45%, p<0.001). At week 64, Ultibro Breezhaler showed numerical improvement over glycopyrronium (LS mean treatment difference 1.95%; p=0.175) and statistical improvement over tiotropium (LS mean treatment difference 4.96%; p=0.001).
COPD exacerbations: In a 64-week study comparing Ultibro Breezhaler (n=729), glycopyrronium (n=739) and tiotropium (n=737), Ultibro Breezhaler reduced the annualised rate of moderate or severe COPD exacerbations by 12% compared to glycopyrronium (p=0.038) and by 10% compared to tiotropium (p=0.096). The number of moderate or severe COPD exacerbations/patient-years was 0.94 for Ultibro Breezhaler (812 events), 1.07 for glycopyrronium (900 events) and 1.06 for tiotropium (898 events). Ultibro Breezhaler also statistically significantly reduced the annualised rate of all COPD exacerbations (mild, moderate or severe) by 15% as compared to glycopyrronium (p=0.001) and 14% as compared to tiotropium (p=0.002). The number of all COPD exacerbations/patient-years was 3.34 for Ultibro Breezhaler (2,893 events), 3.92 for glycopyrronium (3,294 events) and 3.89 for tiotropium (3,301 events).
In the 52-week study comparing Ultibro Breezhaler (n=1,675) and fluticasone/salmeterol (n=1,679), Ultibro Breezhaler met the primary study objective of non-inferiority in rate of all COPD exacerbations (mild, moderate or severe) compared to fluticasone/salmeterol. The number of all COPD exacerbations/patient-years was 3.59 for Ultibro Breezhaler (4,531 events) and 4.03 for fluticasone/salmeterol (4,969 events). Ultibro Breezhaler further showed superiority in reducing the annualised rate of all exacerbations by 11% versus fluticasone/salmeterol (p=0.003).
Compared to fluticasone/salmeterol, Ultibro Breezhaler reduced the annualised rate of both moderate or severe exacerbations by 17% (p<0.001), and of severe exacerbations (requiring hospitalisation) by 13% (not statistically significant, p=0.231). The number of moderate or severe COPD exacerbations/patient-years was 0.98 for Ultibro Breezhaler (1,265 events) and 1.19 for fluticasone/salmeterol (1,452 events). Ultibro Breezhaler prolonged time to first moderate or severe exacerbation with a 22% reduction in risk of an exacerbation (p<0.001) and prolonged time to first severe exacerbation with a 19% reduction in risk of an exacerbation (p=0.046).
The incidence of pneumonia was 3.2% in the Ultibro Breezhaler arm compared to 4.8% in the fluticasone/salmeterol arm (p=0.017). Time to first pneumonia was prolonged with Ultibro Breezhaler compared to fluticasone/salmeterol (p=0.013).
In another study comparing Ultibro Breezhaler (n=258) and fluticasone/salmeterol (n=264), for 26 weeks, the number of moderate or severe COPD exacerbations/patient-years was 0.15 versus 0.18 (18 events versus 22 events), respectively (p=0.512), and the number of all COPD exacerbations/patients-years (mild, moderate or severe) was 0.72 versus 0.94 (86 events versus 113 events), respectively (p=0.098).
Use of rescue medication: Over 26 weeks, Ultibro Breezhaler statistically significantly reduced the use of rescue medication (salbutamol) by 0.96 puffs per day (p<0.001) compared to placebo, 0.54 puffs per day (p<0.001) compared to tiotropium and 0.39 puffs per day (p=0.019) compared to fluticasone/salmeterol. Over 64 weeks, this reduction was 0.76 puffs per day (p<0.001) compared to tiotropium. Over 52 weeks, Ultibro Breezhaler reduced the use of rescue medication by 0.25 puffs per day compared to fluticasone/salmeterol (p<0.001).
Exercise tolerance: Ultibro Breezhaler, dosed in the morning, reduced dynamic hyperinflation and improved the length of time exercise could be maintained from the first dose onwards. On the first day of treatment, inspiratory capacity under exercise was significantly improved (LS mean treatment difference 250 ml, p<0.001) compared to placebo. After three weeks of treatment, the improvement in inspiratory capacity with Ultibro Breezhaler was greater (LS mean treatment difference 320 ml, p<0.001) and exercise endurance time increased (LS mean treatment difference 59.5 seconds, p=0.006) compared to placebo.
Pharmacokinetics: Absorption: Ultibro Breezhaler: Following inhalation of Ultibro Breezhaler, the median time to reach peak plasma concentrations of indacaterol and glycopyrronium was approximately 15 minutes and 5 minutes, respectively.
Based on the in vitro performance data, the dose of indacaterol delivered to the lung is expected to be similar for Ultibro Breezhaler and indacaterol monotherapy product. Steady-state exposure to indacaterol after Ultibro Breezhaler inhalation was either similar or slightly lower than systemic exposure after indacaterol monotherapy product inhalation.
Following inhalation of Ultibro Breezhaler, the absolute bioavailability of indacaterol has been estimated to range from 61 to 85% of the delivered dose, and that of glycopyrronium was about 47% of the delivered dose.
Steady-state exposure to glycopyrronium after Ultibro Breezhaler inhalation was similar to systemic exposure after glycopyrronium monotherapy product inhalation.
Indacaterol: Steady-state concentrations of indacaterol were achieved within 12 to 15 days following once-daily administration. The mean accumulation ratio of indacaterol, i.e. AUC over the 24-h dosing interval on day 14 or day 15 compared to day 1, was in the range of 2.9 to 3.8 for once-daily inhaled doses between 60 micrograms and 480 micrograms (delivered dose).
Glycopyrronium: In patients with COPD, pharmacokinetic steady-state of glycopyrronium was reached within one week of the start of treatment. The steady-state mean peak and trough plasma concentrations of glycopyrronium at the recommended once-daily dosing regimen were 166 picograms/ml and 8 picograms/ml, respectively. Steady-state exposure to glycopyrronium (AUC over the 24-hour dosing interval) was about 1.4- to 1.7-fold higher than after the first dose.
Distribution: Indacaterol: After intravenous infusion, the volume of distribution of indacaterol during the terminal elimination phase was 2557 litres indicating an extensive distribution. The in vitro human serum and plasma protein binding was about 95%.
Glycopyrronium: After intravenous dosing, the steady-state volume of distribution of glycopyrronium was 83 litres and the volume of distribution in the terminal phase was 376 litres. The apparent volume of distribution in the terminal phase following inhalation was almost 20-fold larger, which reflects the much slower elimination after inhalation. The in vitro human plasma protein binding of glycopyrronium was 38% to 41% at concentrations of 1 to 10 nanograms/ml.
Biotransformation: Indacaterol: After oral administration of radiolabelled indacaterol in a human ADME (absorption, distribution, metabolism, excretion) study, unchanged indacaterol was the main component in serum, accounting for about one third of total drug-related AUC over 24 hours. A hydroxylated derivative was the most prominent metabolite in serum. Phenolic O-glucuronides of indacaterol and hydroxylated indacaterol were further prominent metabolites. A diastereomer of the hydroxylated derivative, a N-glucuronide of indacaterol, and C- and N-dealkylated products were further metabolites identified.
In vitro the UGT1A1 isoform is a major contributor to the metabolic clearance of indacaterol. However, as shown in a clinical study in populations with different UGT1A1 genotypes, systemic exposure to indacaterol is not significantly affected by the UGT1A1-genotype.
Oxidative metabolites were found in incubations with recombinant CYP1A1, CYP2D6, and CYP3A4. CYP3A4 is concluded to be the predominant isoenzyme responsible for hydroxylation of indacaterol. In vitro investigations further indicated that indacaterol is a low affinity substrate for the efflux pump P-gp.
Glycopyrronium: In vitro metabolism studies showed consistent metabolic pathways for glycopyrronium bromide between animals and humans. Hydroxylation resulting in a variety of mono- and bis-hydroxylated metabolites and direct hydrolysis resulting in the formation of a carboxylic acid derivative (M9) were seen. In vivo, M9 is formed from the swallowed dose fraction of inhaled glycopyrronium bromide. Glucuronide and/or sulfate conjugates of glycopyrronium were found in urine of humans after repeated inhalation, accounting for about 3% of the delivered dose.
Multiple CYP isoenzymes contribute to the oxidative biotransformation of glycopyrronium. Inhibition or induction of the metabolism of glycopyrronium is unlikely to result in a relevant change of systemic exposure to the active substance.
In vitro inhibition studies demonstrated that glycopyrronium bromide has no relevant capacity to inhibit CYP1A2, CYP2A6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP2E1 or CYP3A4/5, the efflux transporters MDR1, MRP2 or MXR, and the uptake transporters OCT1 or OCT2. In vitro enzyme induction studies did not indicate a clinically relevant induction by glycopyrronium bromide for any of the cytochrome P450 isoenzymes tested or for UGT1A1 and the transporters MDR1 and MRP2.
Elimination: Indacaterol: In clinical studies, the amount of indacaterol excreted unchanged via urine was generally lower than 2.5% of the delivered dose. Renal clearance of indacaterol was, on average, between 0.46 and 1.2 litres/hour. When compared with the serum clearance of indacaterol of 23.3 litres/hour, it is evident that renal clearance plays a minor role (about 2 to 5% of systemic clearance) in the elimination of systemically available indacaterol.
In a human ADME study, indacaterol given orally was excreted into human faeces primarily as unchanged parent substance (54% of the dose) and, to a lesser extent, hydroxylated indacaterol metabolites (23% of the dose).
Indacaterol serum concentrations declined in a multi-phasic manner with an average terminal half-life ranging from 45.5 to 126 hours. The effective half-life, calculated from the accumulation of indacaterol after repeated dosing ranged from 40 to 52 hours which is consistent with the observed time-to-steady state of approximately 12-15 days.
Glycopyrronium: After intravenous administration of [3H]-labelled glycopyrronium bromide, the mean urinary excretion of radioactivity in 48 hours amounted to 85% of the dose. A further 5% of the dose was found in the bile.
Renal elimination of parent drug accounts for about 60 to 70% of total clearance of systemically available glycopyrronium whereas non-renal clearance accounts for about 30 to 40%. Biliary clearance contributes to the non-renal clearance, but the majority of non-renal clearance is thought to be due to metabolism.
Mean renal clearance of glycopyrronium following inhalation was in the range of 17.4 and 24.4 litres/h. Active tubular secretion contributes to the renal elimination of glycopyrronium. Up to 23% of the delivered dose was found in urine as parent drug.
Glycopyrronium plasma concentrations declined in a multi-phasic manner. The mean terminal elimination half-life was much longer after inhalation (33 to 57 hours) than after intravenous (6.2 hours) and oral (2.8 hours) administration. The elimination pattern suggests sustained lung absorption and/or transfer of glycopyrronium into the systemic circulation at and beyond 24 h after inhalation.
Linearity/non-linearity: Indacaterol: Systemic exposure to indacaterol increased with increasing (delivered) dose (120 micrograms to 480 micrograms) in a dose proportional manner.
Glycopyrronium: In COPD patients, both systemic exposure and total urinary excretion of glycopyrronium at pharmacokinetic steady-state increased about dose-proportionally over the (delivered) dose range of 44 to 176 micrograms.
Special populations: Ultibro Breezhaler: A population pharmacokinetic analysis of data in COPD patients after inhalation of Ultibro Breezhaler indicated no significant effect of age, gender and (lean body) weight on the systemic exposure to indacaterol and glycopyrronium. Lean body weight (which is a function of weight and height) was identified as a covariate. A negative correlation between systemic exposure and lean body weight (or body weight) was observed; however, no dose adjustment is recommended due to the magnitude of the change or the predictive precision of lean body weight.
Smoking status and baseline FEV1 had no apparent effect on systemic exposure to indacaterol and glycopyrronium after inhalation of Ultibro Breezhaler.
Indacaterol: A population pharmacokinetic analysis showed that there is no clinically relevant effect of age (adults up to 88 years), sex, weight (32-168 kg) or race on the pharmacokinetics of indacaterol. It did not suggest any difference between ethnic subgroups in this population.
Glycopyrronium: A population pharmacokinetic analysis of data in COPD patients identified body weight and age as factors contributing to inter-patient variability in systemic exposure. Glycopyrronium at the recommended dose can be safely used in all age and body weight groups.
Gender, smoking status and baseline FEV1 had no apparent effect on systemic exposure.
Patients with hepatic impairment: Ultibro Breezhaler: Based on the clinical pharmacokinetic characteristics of its monotherapy components, Ultibro Breezhaler can be used at the recommended dose in patients with mild and moderate hepatic impairment. No data are available for subjects with severe hepatic impairment.
Indacaterol: Patients with mild and moderate hepatic impairment showed no relevant changes in Cmax or AUC of indacaterol, nor did protein binding differ between mild and moderate hepatic impaired subjects and their healthy controls. Studies in subjects with severe hepatic impairment were not performed.
Glycopyrronium: Clinical studies have not been conducted in patients with hepatic impairment. Glycopyrronium is cleared predominantly from the systemic circulation by renal excretion. Impairment of the hepatic metabolism of glycopyrronium is not thought to result in a clinically relevant increase of systemic exposure.
Patients with renal impairment: Ultibro Breezhaler: Based on the clinical pharmacokinetic characteristics of its monotherapy components, Ultibro Breezhaler can be used at the recommended dose in patients with mild to moderate renal impairment. In patients with severe renal impairment or end-stage renal disease requiring dialysis, Ultibro Breezhaler should be used only if the expected benefit outweighs the potential risk.
Indacaterol: Due to the very low contribution of the urinary pathway to total body elimination of indacaterol maleate, a study in renal impaired subjects was not performed.
Glycopyrronium: Renal impairment has an impact on the systemic exposure to glycopyrronium bromide. A moderate mean increase in total systemic exposure (AUClast) of up to 1.4-fold was seen in subjects with mild and moderate renal impairment and up to 2.2-fold in subjects with severe renal impairment and end-stage renal disease. In COPD patients with mild and moderate renal impairment (estimated glomerular filtration rate, eGFR ≥30 ml/min/1.73 m2) glycopyrronium bromide can be used at the recommended dose.
Ethnicity: Ultibro Breezhaler: There were no major differences in total systemic exposure (AUC) for both compounds between Japanese and Caucasian subjects. Insufficient pharmacokinetic data is available for other ethnicities or races.
Indacaterol: No difference between ethnic subgroups was identified. Limited treatment experience is available for the Black population.
Glycopyrronium: There were no major differences in total systemic exposure (AUC) between Japanese and Caucasian subjects. Insufficient pharmacokinetic data is available for other ethnicities or races.
Toxicology: Preclinical safety data: Ultibro Breezhaler: Pre-clinical studies included in vitro and in vivo safety pharmacology assessments, repeated-dose inhalation toxicity studies in rats and dogs and an inhalation embryo-foetal development study in rats.
Increased heart rates were apparent in dogs at all doses of Ultibro Breezhaler and each monotherapy component. The effects on heart rate for Ultibro Breezhaler increased in magnitude and duration when compared with the changes observed for each component alone consistent with an additive response. Shortening of electrocardiograph intervals and decreased systolic and diastolic blood pressure were also apparent. Indacaterol administered to dogs alone or in Ultibro Breezhaler was associated with a similar incidence and severity of myocardial lesions. Systemic exposures (AUC) at the no-observed-adverse-effect level (NOAEL) for myocardial lesions were 64- and 59-fold higher than in humans, for each component, respectively.
No effects on the embryo or foetus were seen at any dose level of Ultibro Breezhaler during an embryo-foetal development study in rats. Systemic exposures (AUC) at the no-observed-adverse-effect level (NOAEL) were 79- and 126-fold higher than in humans, for indacaterol and glycopyrronium, respectively.
Indacaterol: Effects on the cardiovascular system attributable to the beta2-agonistic properties of indacaterol included tachycardia, arrhythmias and myocardial lesions in dogs. Mild irritancy of the nasal cavity and larynx were seen in rodents. All these findings occurred at exposures sufficiently in excess of those anticipated in humans.
Although indacaterol did not affect general reproductive performance in a rat fertility study, a decrease in the number of pregnant F1 offspring was observed in the peri- and post-developmental rat study at an exposure 14-fold higher than in humans treated with indacaterol. Indacaterol and its metabolites transferred rapidly into the milk of lactating rats. Indacaterol was not embryotoxic or teratogenic in rats or rabbits.
Genotoxicity studies did not reveal any mutagenic or clastogenic potential. Carcinogenicity was assessed in a two-year rat study and a six-month transgenic mouse study. Increased incidences of benign ovarian leiomyoma and focal hyperplasia of ovarian smooth muscle in rats were consistent with similar findings reported for other beta2-adrenergic agonists. No evidence of carcinogenicity was seen in mice. Systemic exposures (AUC) in rats and mice at the no-observed-adverse-effect levels in these studies were at least 7- and 49-fold higher, respectively, than in humans treated with indacaterol once a day at the maximum recommended therapeutic dose.
Glycopyrronium: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction and development.
Effects attributable to the muscarinic receptor antagonist properties of glycopyrronium bromide included mild to moderate increases in heart rate in dogs, lens opacities in rats and, reversible changes associated with reduced glandular secretions in rats and dogs. Mild irritancy or adaptive changes in the respiratory tract were seen in rats. All these findings occurred at exposures sufficiently in excess of those anticipated in humans.
Glycopyrronium was not teratogenic in rats or rabbits following inhalation administration. Fertility and pre- and post-natal development were not affected in rats. Glycopyrronium bromide and its metabolites did not significantly cross the placental barrier of pregnant mice, rabbits and dogs. Glycopyrronium bromide (including its metabolites) was excreted into the milk of lactating rats and reached up to 10-fold higher concentrations in the milk than in the blood of the dam.
Genotoxicity studies did not reveal any mutagenic or clastogenic potential for glycopyrronium bromide. Carcinogenicity studies in transgenic mice using oral administration and in rats using inhalation administration revealed no evidence of carcinogenicity at systemic exposures (AUC) of approximately 53-fold higher in mice and 75-fold higher in rats than the maximum recommended dose once daily for humans.